Description:
A 56yrs old patient was considered to evaluate a chronic Broncho-esophageal fistula for last 4 years, perhaps secondary to eroded TB nodes in the past as she has received ATT in the past. Recent CT with oral contrast confirmed the fistula communicating with with the Lt main bronchus. Patient has constant pulmonary complaints due to that and therefore this evaluation.
-
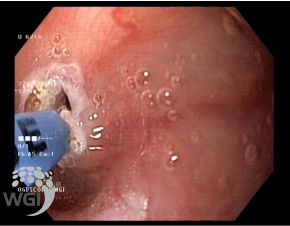
Endoscopy showed a classical bronco-esophageal fistula at 24 cms from the incisors.
-
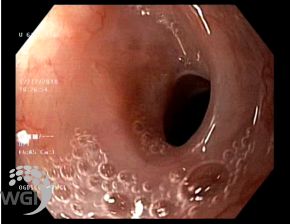
Rest of the upper G.I. tract appeared normal upto the duodenum.
-
Closure of fistula with the help of padlock clip (11 mm). We performed APC for the fistulous opening prior to clipping.
-
Optimal clip placement was confirmed both on endoscopy as well as Fluoroscopy.
-
Gastrograffin studies after few weeks showed complete closure of Broncho-esophageal fistula and no leak of contrast was seen from the esophagus to bronchial tree.
TAKE HOME MESSAGE
This case of a chronic broncho-esophageal fistula was very effectively treated with endoscopic technique with the help of new clip technology. Hence, patient who has developed such complications or has perforations upto 2 cms can be very effectively treated without any formal surgery which was the norm till recently. This case shows us that Endoscopic treatment of vast majority of benign GI conditions should be explored first and only if it is not feasible or safe then surgery should be the last option.
Image:

1. A classical Bronchoesophageal fistula at 24 cms from the incisors

2. Duodenum appeared normal
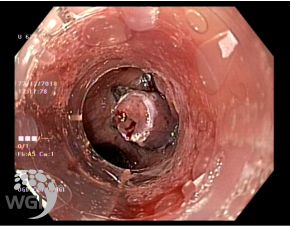
3. A chronic bronchoesophageal fistula
4. We performed APC for the fistulous opening prior to clipping.
5. Optimal clip placement was confirmed on endoscopy

6. Gastrograffin studies showed no leak of contrast was seen from the esophagus to bronchial tree.
Posted by Dr. Vipulroy Rathod
Mar 29, 2019
Categories:
Gastrovision Case Capsules
© Endoscopy Asia