Description:
A 75 yrs female patient was referred to evaluate a suspicious filling defect in the lower CBD seen on USG scan with abnormal LFT. Patient has undergone cholecystectomy elsewhere many years ago. In view of these findings EUS and ERC was considered. EUS revealed normal CBD and gall bladder.
-
EUS revealed dilated CBD 11 mm with an 8 mm stone impacted just above the ampulla of vater in the lower CBD.
-
One large 2.0 cms x 1.2 cms stone impacted in the cystic duct / CBD junction leading to a sort of Mirrizzi’s syndrome.
-
Large cystic duct stump was noted with few small concrements within apart from this large cystic duct stone. Pancreas and MPD appeared normal.
-
ERC was considered Duodenoscopy revealed intra diverticular ampulla. Selective cannulation of bileduct was achieved.
-
Cholangiogram showed large 2.0 cms x 1.2 cms stone impacted in the cystic duct
-
Biliary sphincterotomy was performed and then the small stone extraction was carried out with balloon catheter. followed by balloon dilatation of the cystic duct /CBD junction after passing deep in the cystic duct remanant.
-
Post dilatation the large 2.0 cms stone was then gently extracted with a stone extraction balloon catheter from the cystic duct.
-
Occlusion cholangiogram confirmed complete ductal clearance
-
A 7 fr double pigtail stent was placed in the CBD due to aggressive intervention, to ensure free flow of bile.
TAKE HOME MESSAGE
As we can see in this case, we were able to accurately diagnose presence of stones in the CBD and Cystic duct on EUS. After the clearance of lower CBD stone, we managed to extract 2.0 cms stone from the cystic duct with a unique technique of a wire guided balloon dilatation of the cystic duct/CBD junction followed by conventional balloon catheter stone extraction. Hence, we avoided any need for laser lithotripy with cholangioscopy in this case with modified technique. Again I would like to emphasize, the importance of EUS-ERCP Interface in this case as seen here and we wish that more clinicians will embrace this protocol for optimum care in Pancreato-Biliary disease management.
Image:

1. EUS revealed large 2.0 cms x 1.2 cms stone impacted in the cystic duct
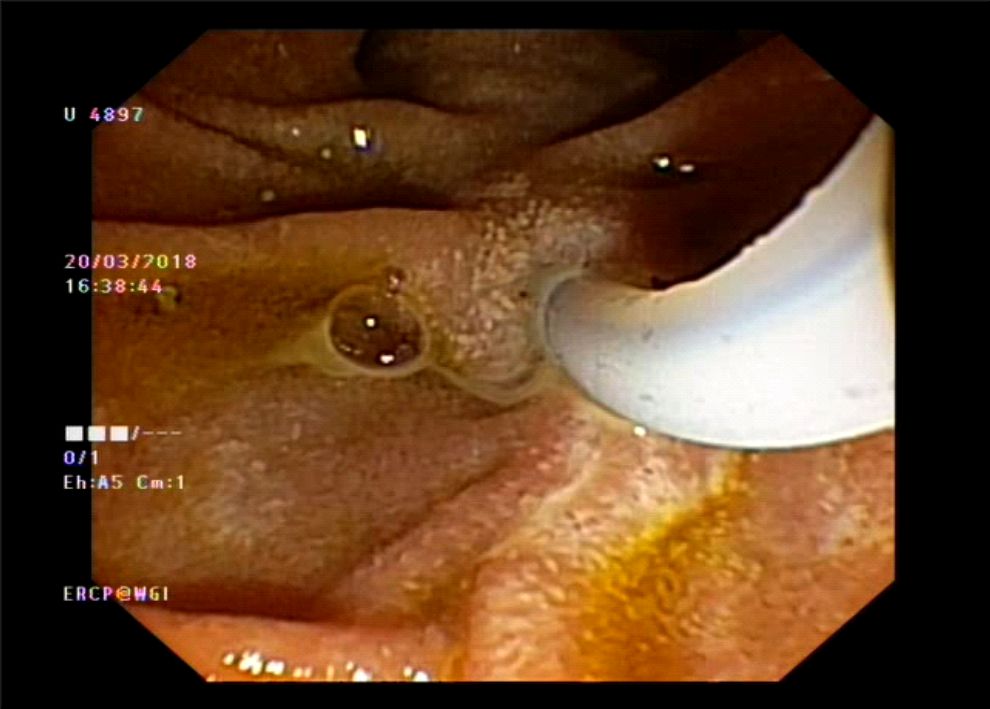
2. Selective cannulation of bile duct
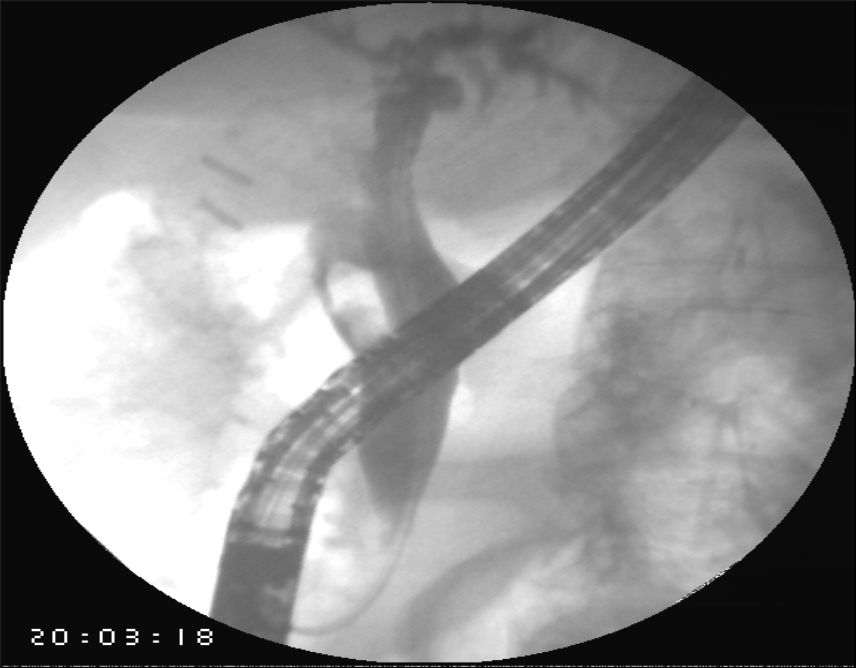
3. Cholangiogram showed large 2.0 cms x 1.2 cms stone impacted in the cystic duct
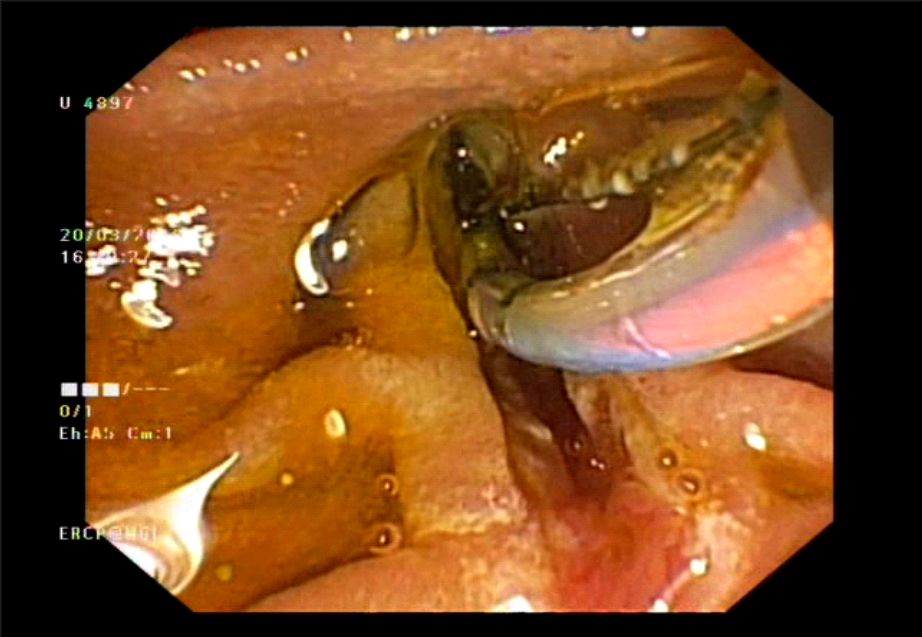
4. Biliary sphincterotomy was performed
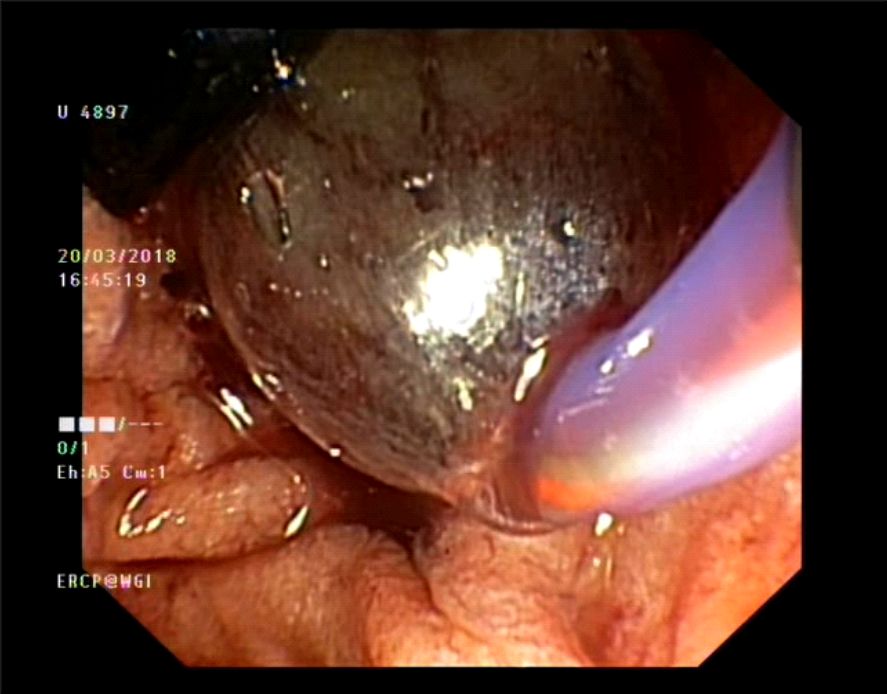
5. Balloon dilatation performed of the lower CBD

6. Large 2.0 cms stone was then extracted from cystic duct with a balloon catheter.

7. Occlusion cholangiogram confirmed complete ductal clearance

8. A 7 fr double pigtail stent was placed to ensure free flow of bile
Posted by Dr. Vipulroy Rathod
Apr 03, 2019
Categories:
Gastrovision Case Capsules
© Endoscopy Asia