Description:
-
A 49 yrs female patient was sent to us for the favor of endoscopic palliation of obstructive jaundice. Patient is a known operated case of CA stomach in the past with Roux-en-y anastomosis
-
Now patient has severe cholangitis and cholestatic symptoms hence endoscopic palliation was considered
-
Endoscopic evaluation of the stomach showed oedematous stomach with patent g-j
-
Scope could be passed across all the loops of roux-en-y anastomosis, but due to a very long afferent loop even enteroscopic ERC was not feasible and hence EUS guided approach was considered
-
EUS showed extensive ascites and few liver mets and large mass and massively dilated system
-
In view of these findings, EUS -guided Hepatico-Gastrostomy was performed
-
EUS showed a dilated left hepatic duct and hence EUS guided needle puncture of the left hepatic duct was performed. The tract was sequentially dilated with cystotomes to facilitate stent placement
-
A self expandable partially covered Giobor stent 10 cms and free flow of infected bile was seen from the stent in the stomach
Take Home Message:
In cases where traditional ERC and biliary stenting is not feasible due to altered anatomy because of surgery or when PTC drainage too is not feasible due to ascites and liver mets, this unique technique of EUS guided Hepatico-gastrostomy allows us to decompress the obstructed biliary system and palliate cholestatic symptoms. First EUS guided Choledochoduodenostomy was performed by us in 2001 and since then the technology and techniques have evolved. Hence, for more than a decade the need for PTC for advanced biliary obstruction is on decline worldwide due to advent of EUS guided biliary drainage.
Image:
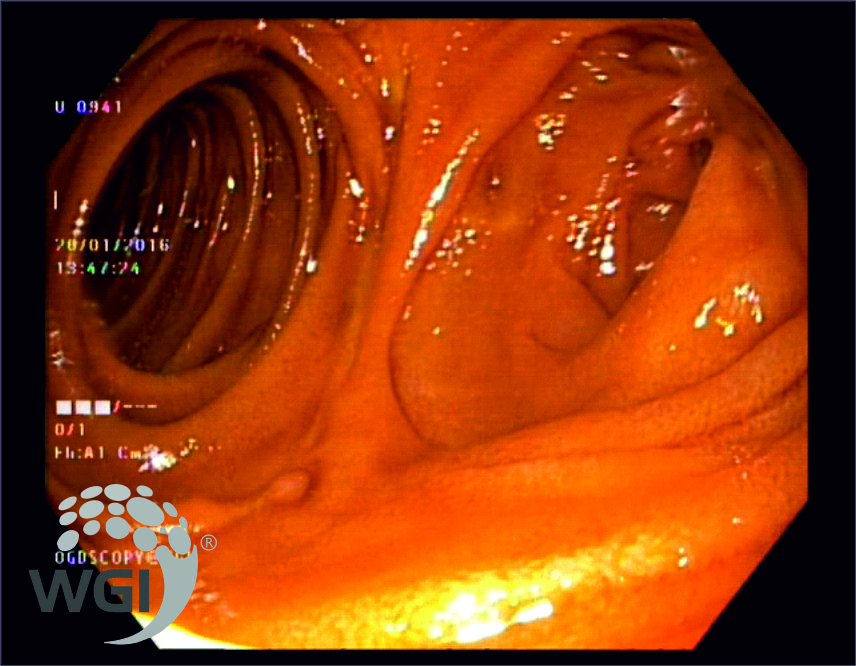
1. Stomach showed edematous with patent G-J
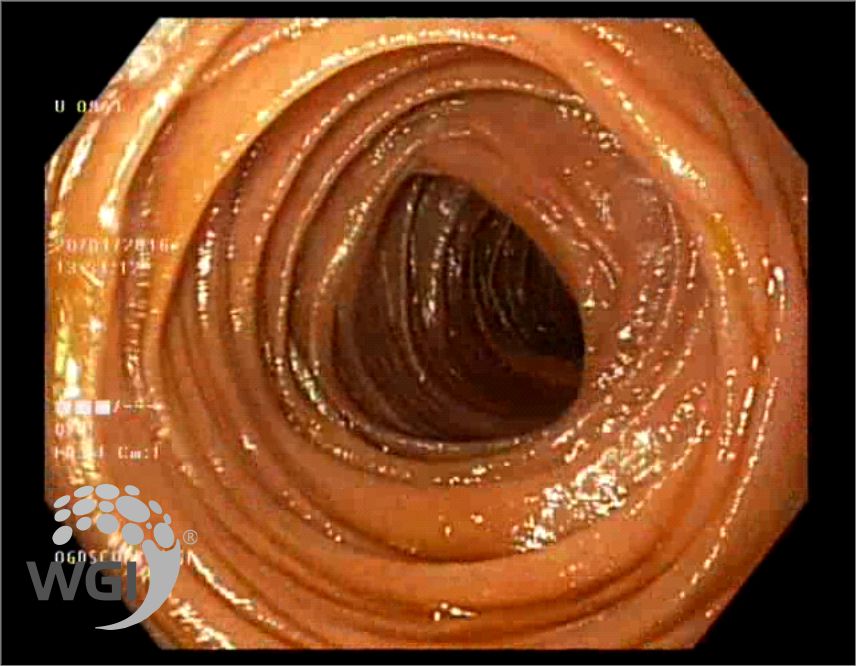
2. Scope could be passed across all the loops of Roux-en-y anastomosis

3. EUS showed extensive ascites and few liver mets
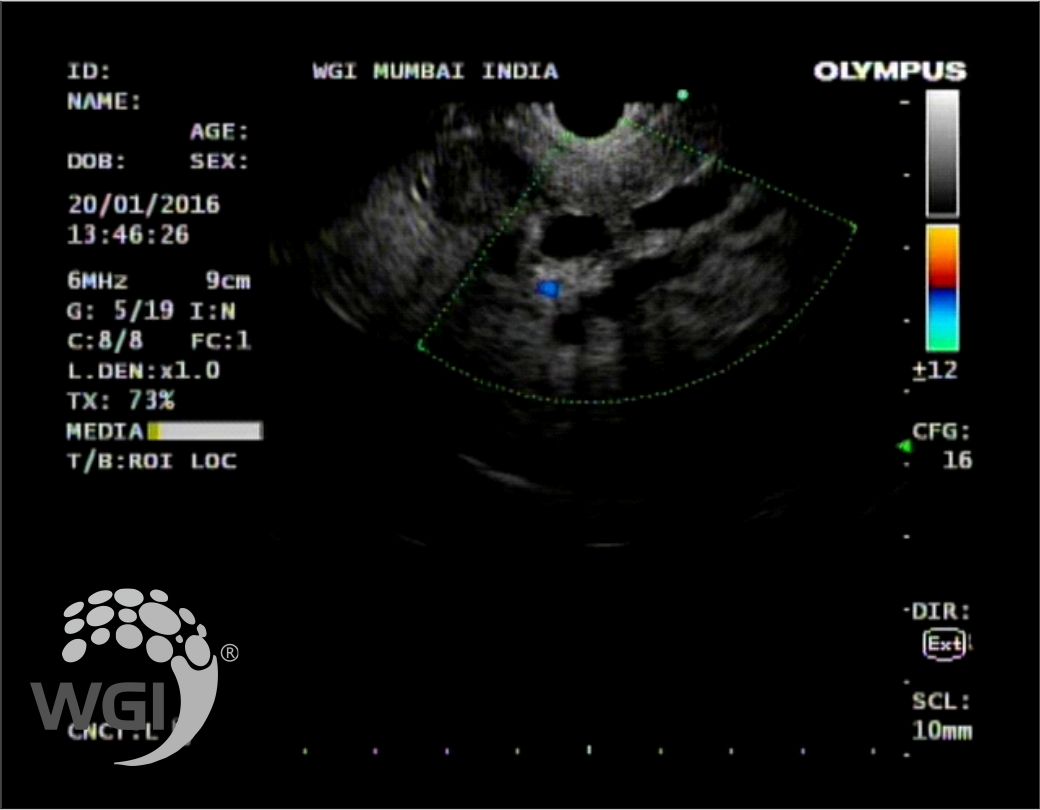
4. EUS showed large mass and massively dilated system

5. EUS-guided hepatico-gastrostomy was performed
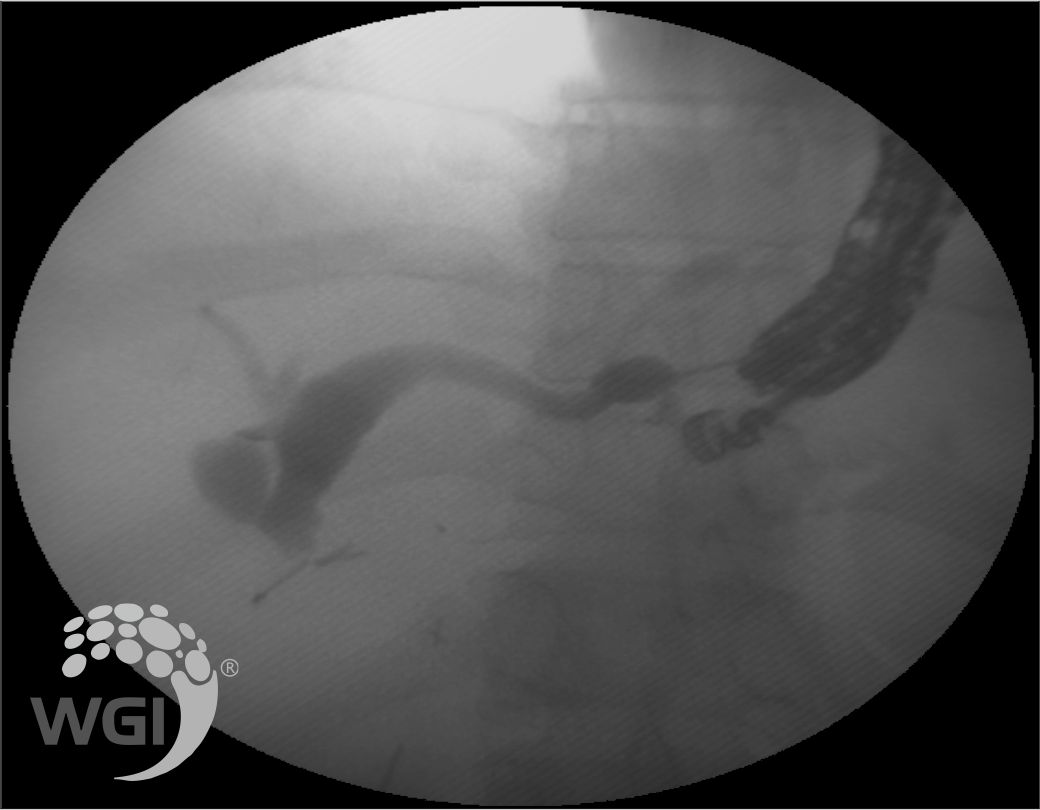
6. Fluoroscopy showed dilated left hepatic duct
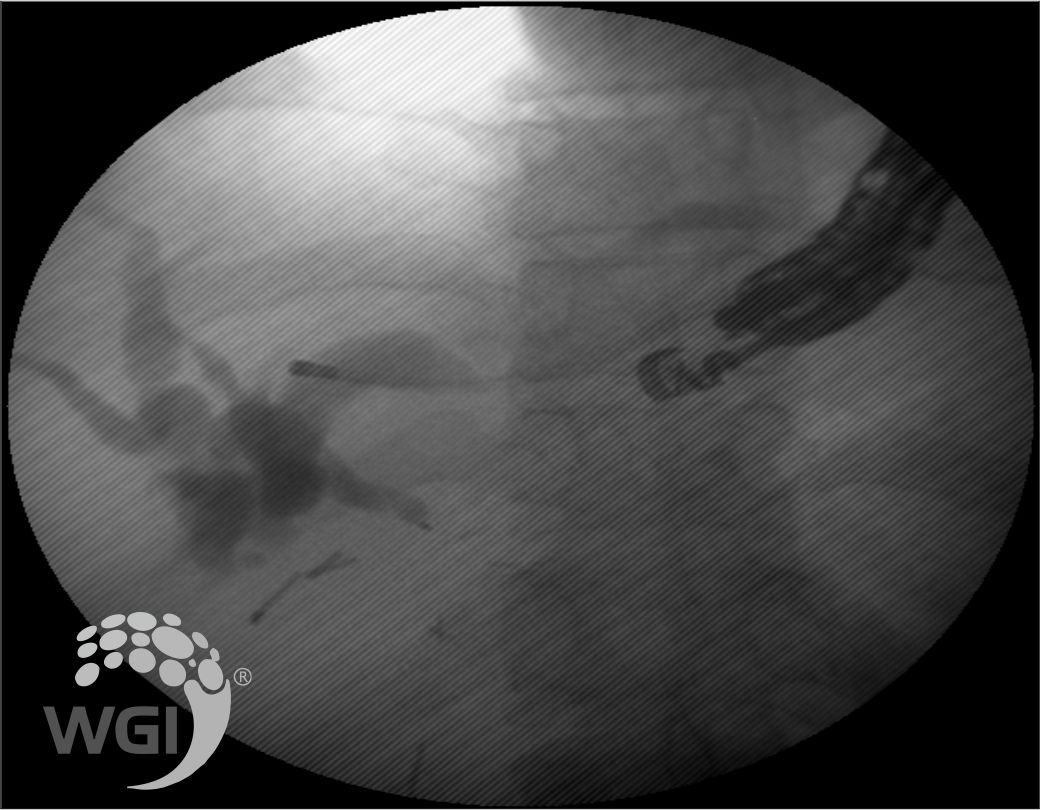
7. Left hepatic duct was punctured and sequentially dilated with cystotome
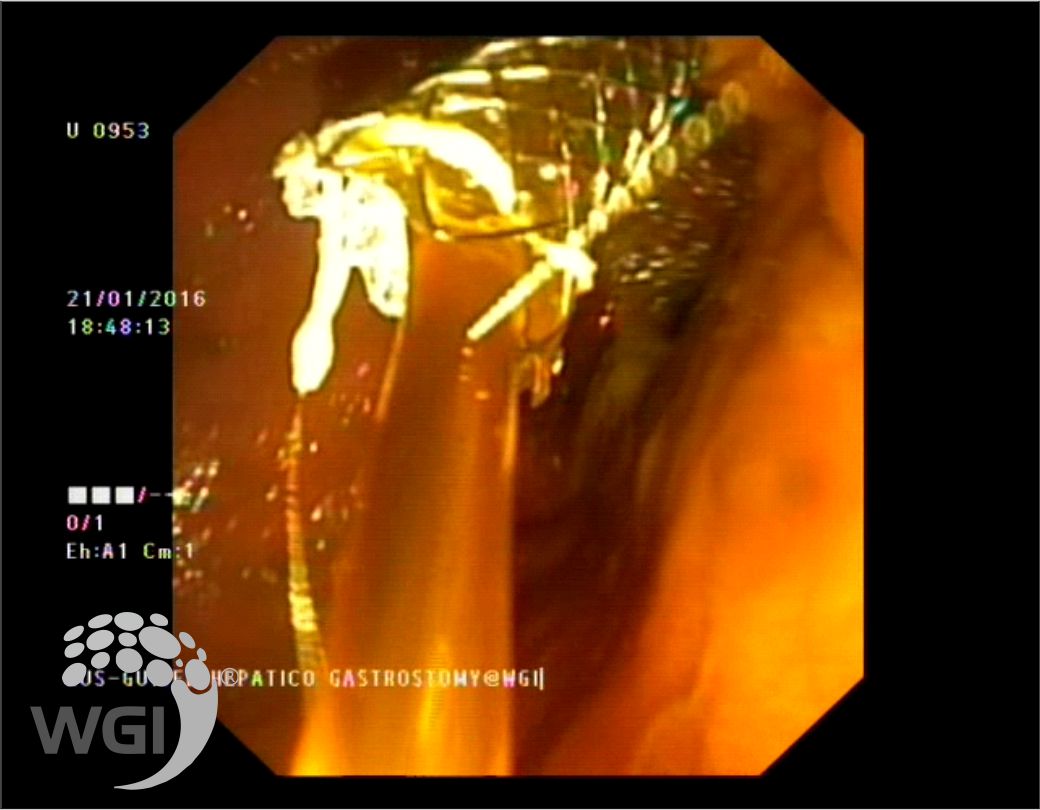
8. A self expandable partially covered Giobor stent 10 cms and free flow of infected bile was seen from the stent.
Posted by Dr. Vipulroy Rathod
Sep 27, 2019
Categories:
Gastrovision Case Capsules
© Endoscopy Asia