Description:
A 55yrs old patient came with complaints of bleeding per rectum off and on as well as altered bowel habits for the last 1 year. Therefore, a colonoscopy was performed to evaluate the exact etiology of bleeding per rectum as well as altered bowel habits.
-
Scope was passed up to terminal ileum, which appeared normal
-
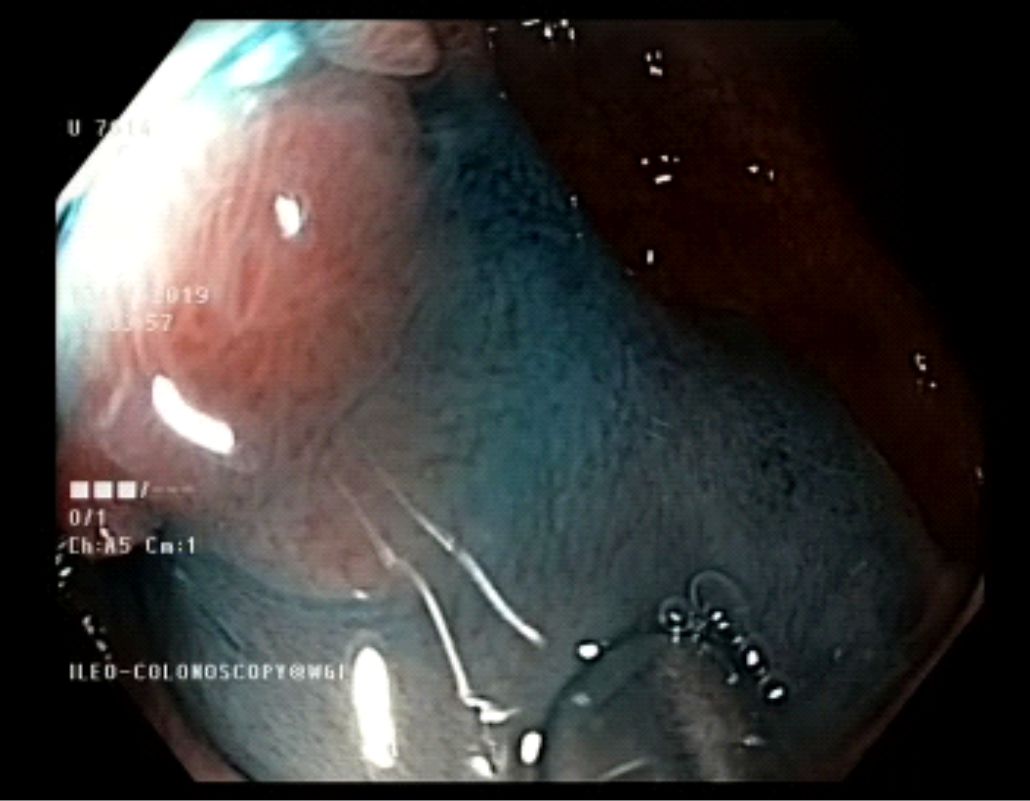
A large 2-3 cms polypoidal lesion was seen in the recto-sigmoid colon which appeared tubulovillous.
-
This large polyp was then removed endoscopically - EMR polypectomy was then performed with injection and snare technique
-
Complete haemostasis was ensured
-
Resected lesion was retrieved and sent for HPE - Histopathology revealed tubulovillous adenoma with high grade dysplasia only
TAKE HOME MESSAGE
As we have seen in this case, a 55 years old male had h/o bleeding per rectum and altered bowel. Colonoscopic evaluation detected a large polyp with high grade dysplasia on HPE. Thus, we avoided a potential full blown cancer of colon due to timely intervention. It is my personal request to all the clinicians to keep this in mind that any patient above the age of 45 years has either bleeding per rectum or altered bowel habits with or without wt loss, they then qualify for a screening colonoscopy.
Furthermore, if there is a family history of colon cancer then definitely the siblings of that patient and children will require a screening colonoscopy after the age of 45 years. At WGI, we performed Endoscopic Mucosal Resection (EMR), Endoscopic Submucosal Dissection (ESD) and we have recently introduced a new device called OVESCO FTRD (full thickness resection device) for those lesions beyond the submucosal layer.
Advanced Endoscopy has evolved in such a big way in the last few decades that in the USA due to screening colonoscopy there has been a 50% reduction of elective surgery for colo-rectal cancers. We foresee that in the coming decades, that only 10% patients will require surgery. This case is to highlight the importance of screening colon cancer in high risk groups of patients.
Image:
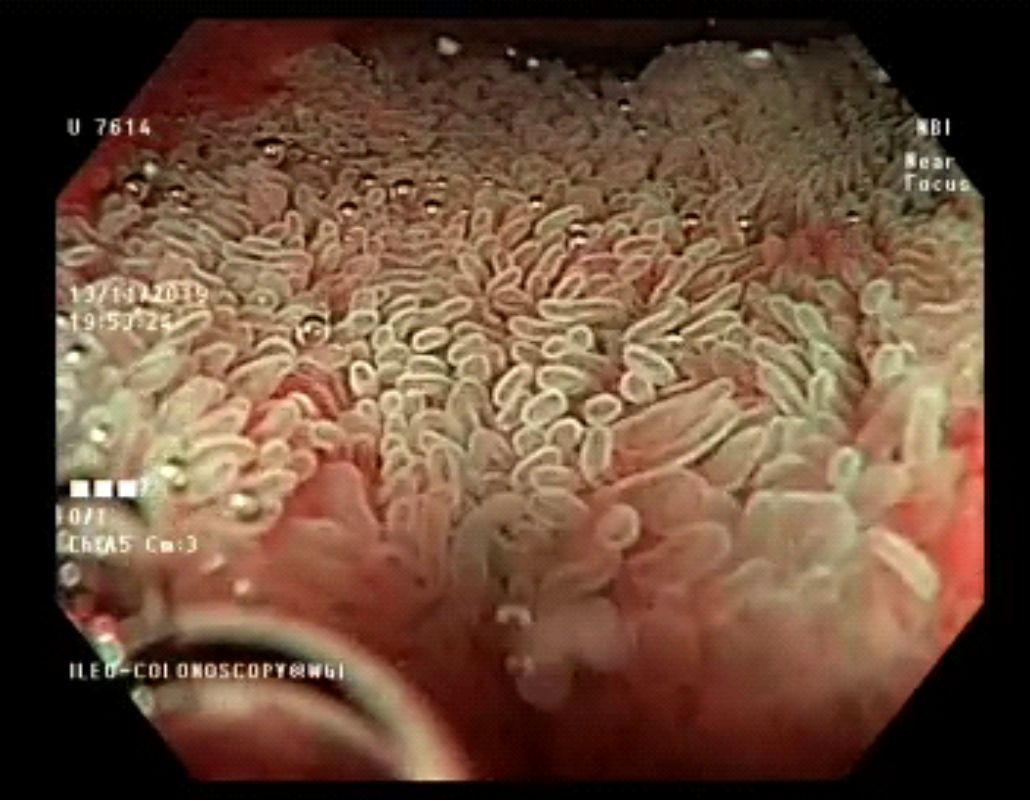
1. Scope was passed up to terminal ileum
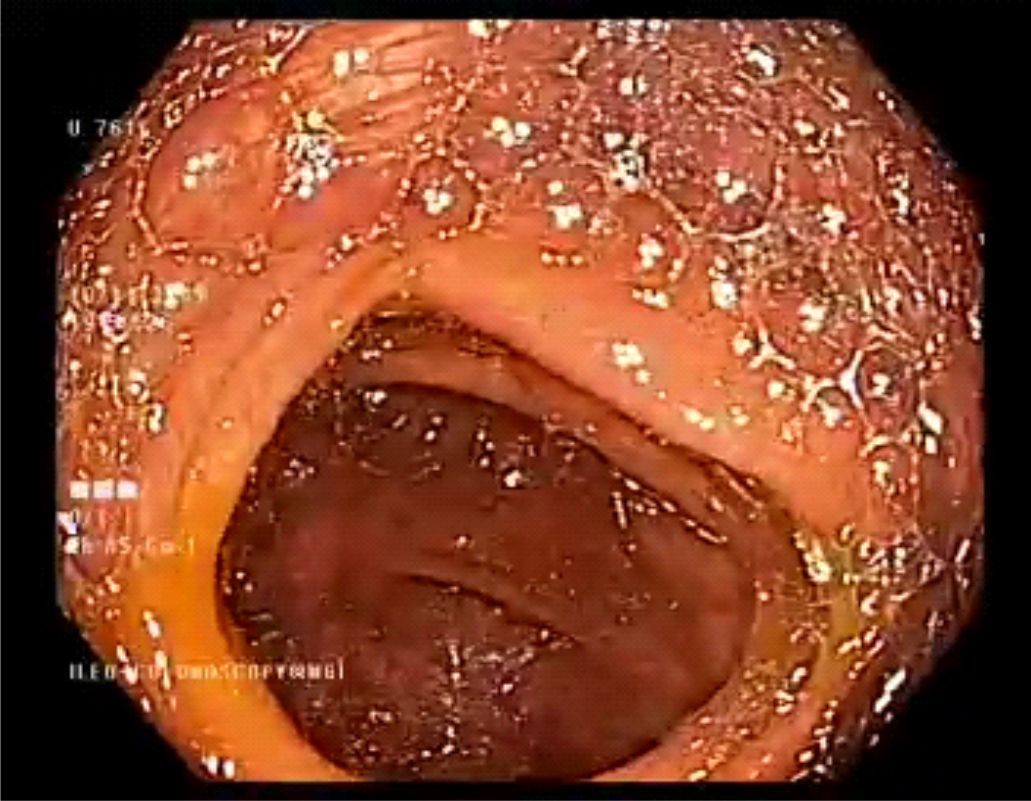
2. Caecum
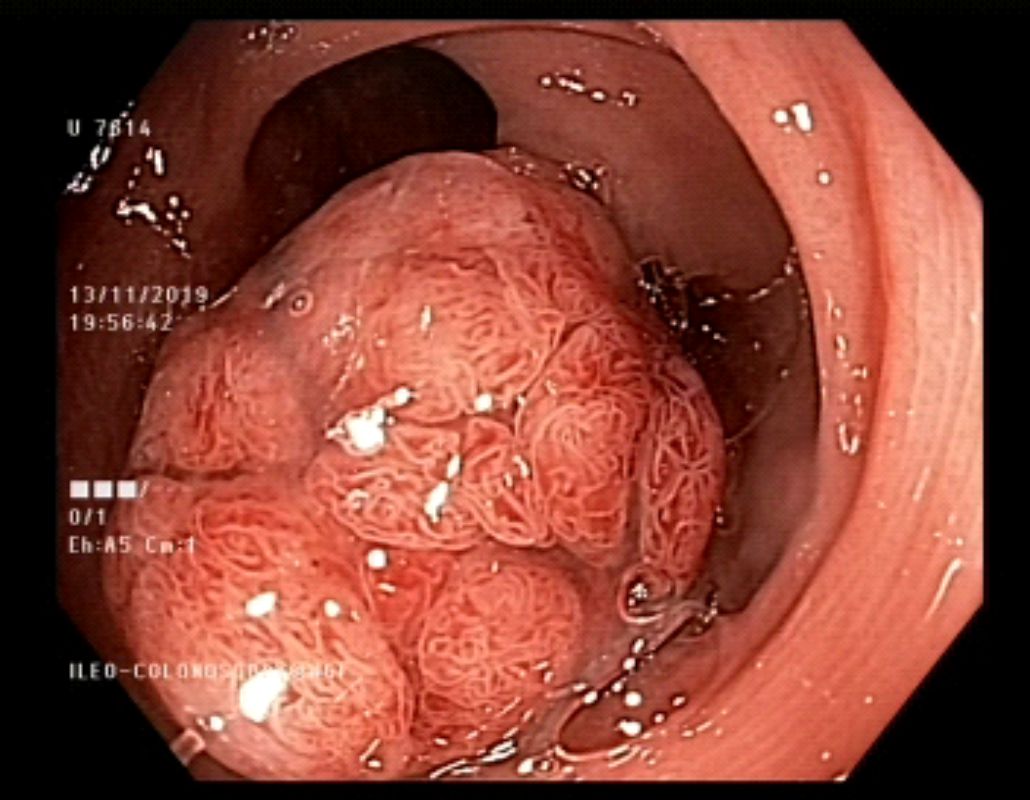
3. 2-3 cms polypoidal lesion was seen in the recto-sigmoid colonwhich appeared tubulovillous
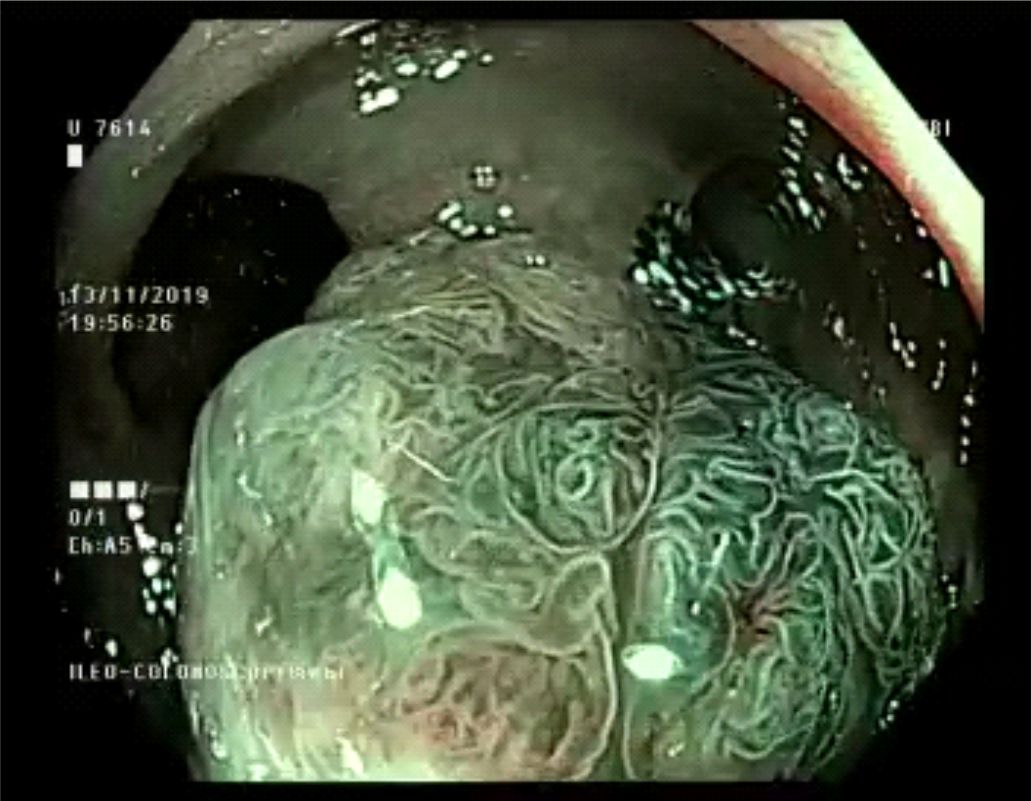
4. Magnification endoscopy and NBI it certainly appeared tubulovillous
5. The polyp is lifted from underlying tissue using a fluid injection
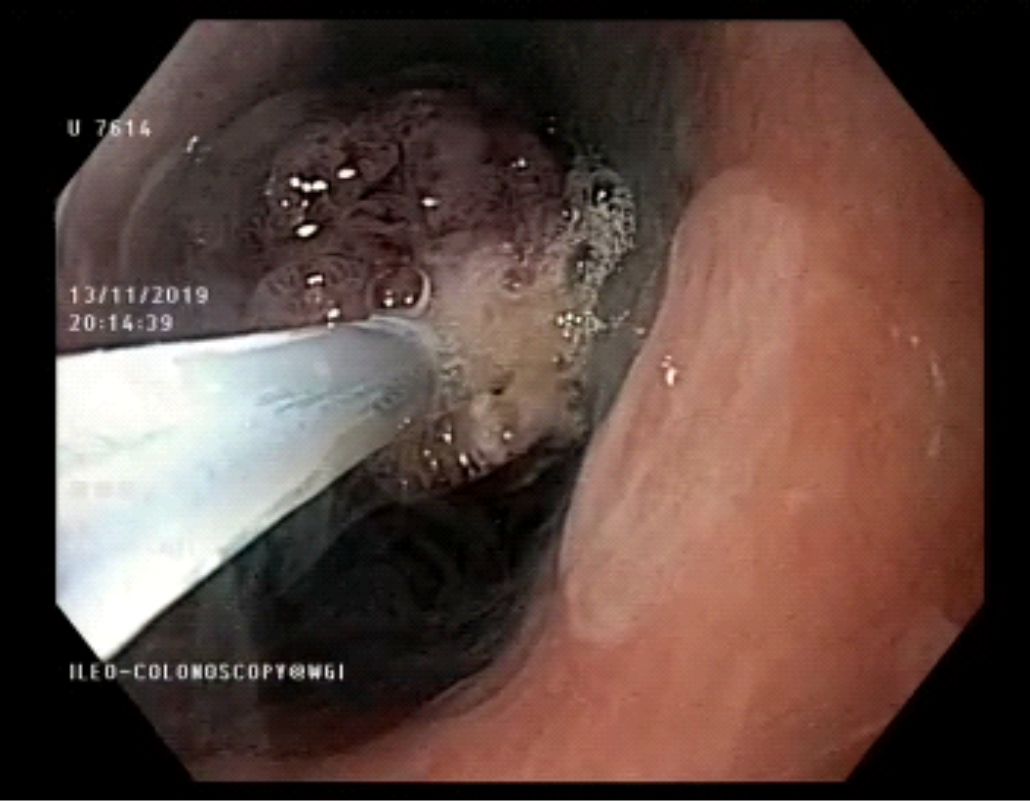
6. EMR polypectomy was then performed with snare technique
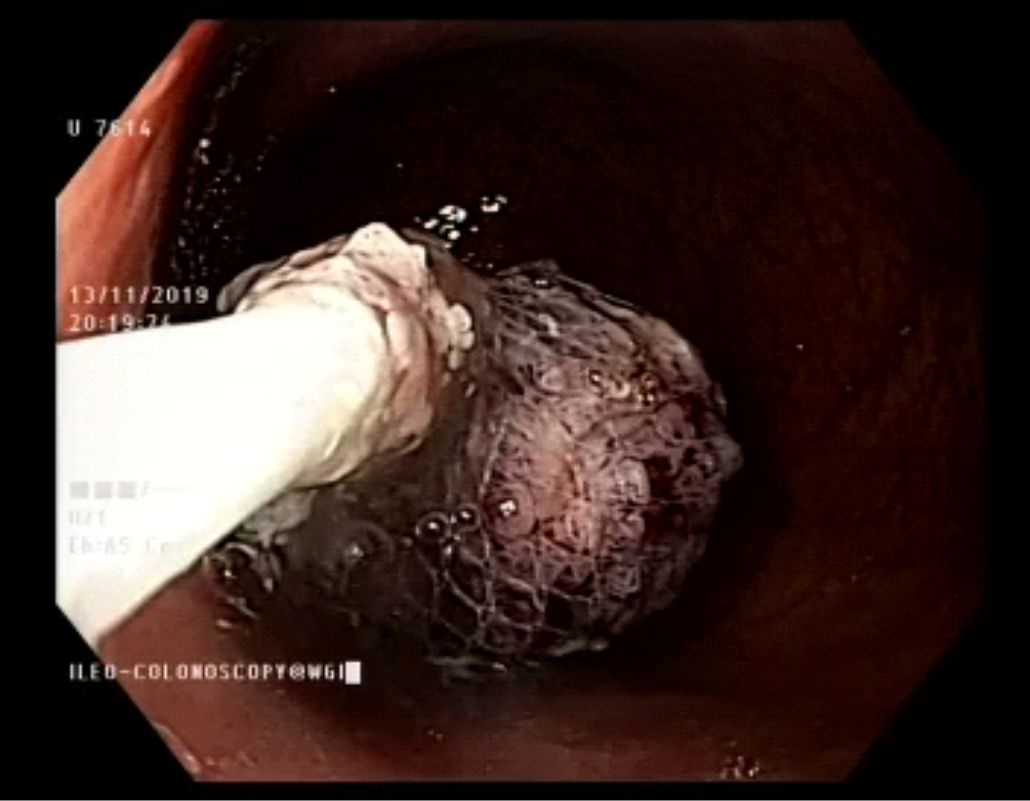
7. Resected lesion was retrieved
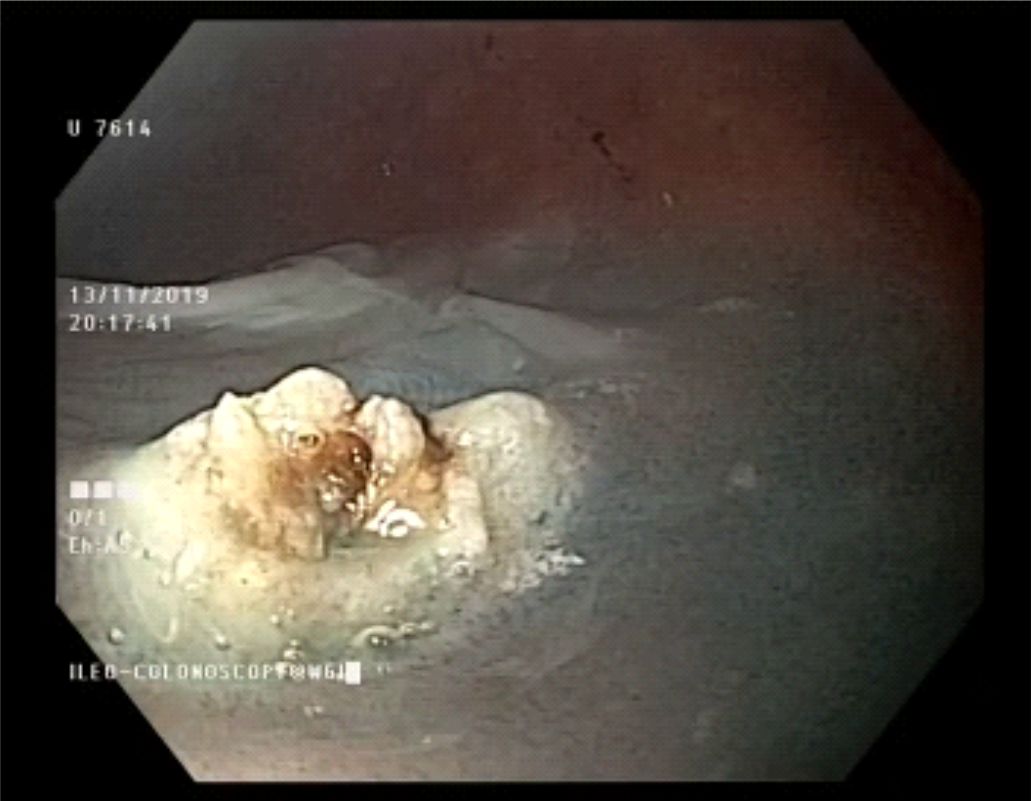
8. Complete haemostasis was ensured
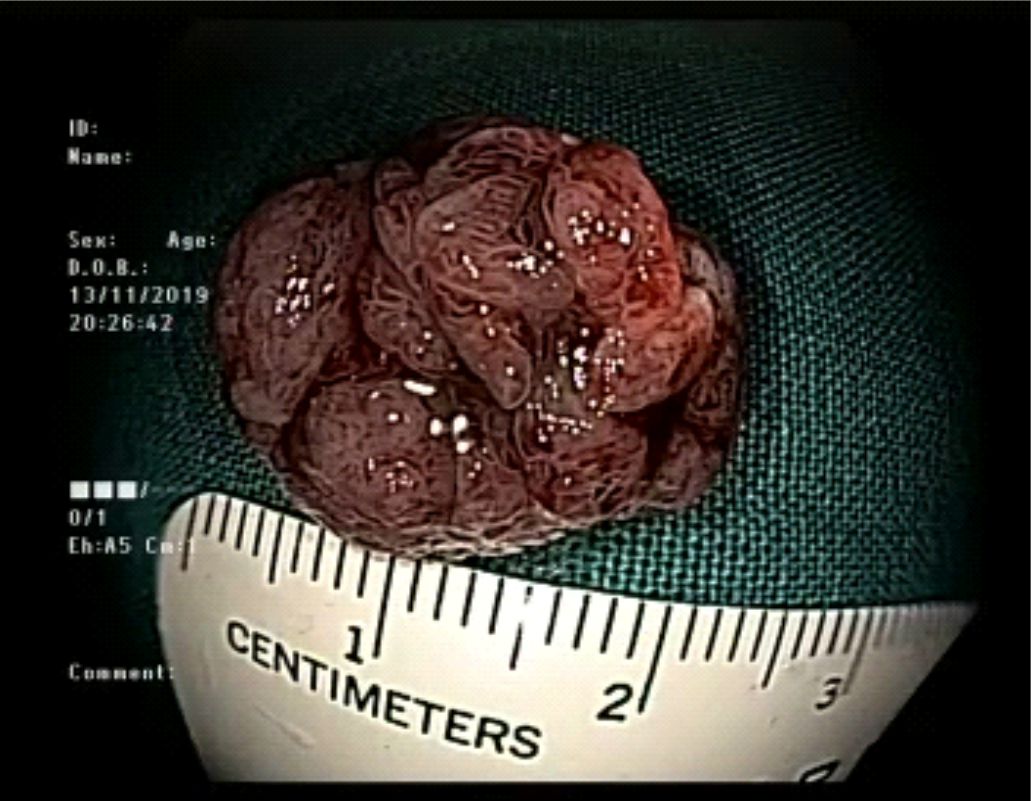
9. Resected lesion
Posted by Dr. Vipulroy Rathod
Jan 05, 2020
Categories:
Gastrovision Case Capsules
© Endoscopy Asia